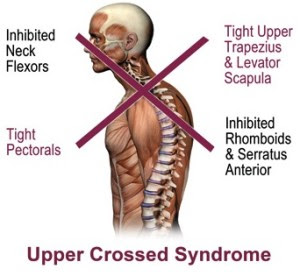
Upper Cross Syndrome is a postural imbalance pattern, Crossed pattern of muscle tightness and weakness. Muscle balance can be defined as a relative equality of muscle length or strength between an agonist and an antagonist; this balance is necessary for normal movement and function[4].Muscle imbalance usually occurs before functional dysfunction[11]. The condition in which few muscles undergo inhibition and become weak while others become short and stiff can bring certain changes in the tissues which may cause inappropriate movement patterns.
- Tightness in the upper trapezius, levator scapulae, Sternocleidomastoid and pectoralis major/minor
- Weakness in the deep cervical flexors, lower trapezius, Rhomboids and serratus anterior
| Main Postural Issues |
| Forward head posture, rounded shoulders, cervical lordosis, thoracic kyphosis |
Associated Terms- Proximal or shoulder girdle crossed syndrome
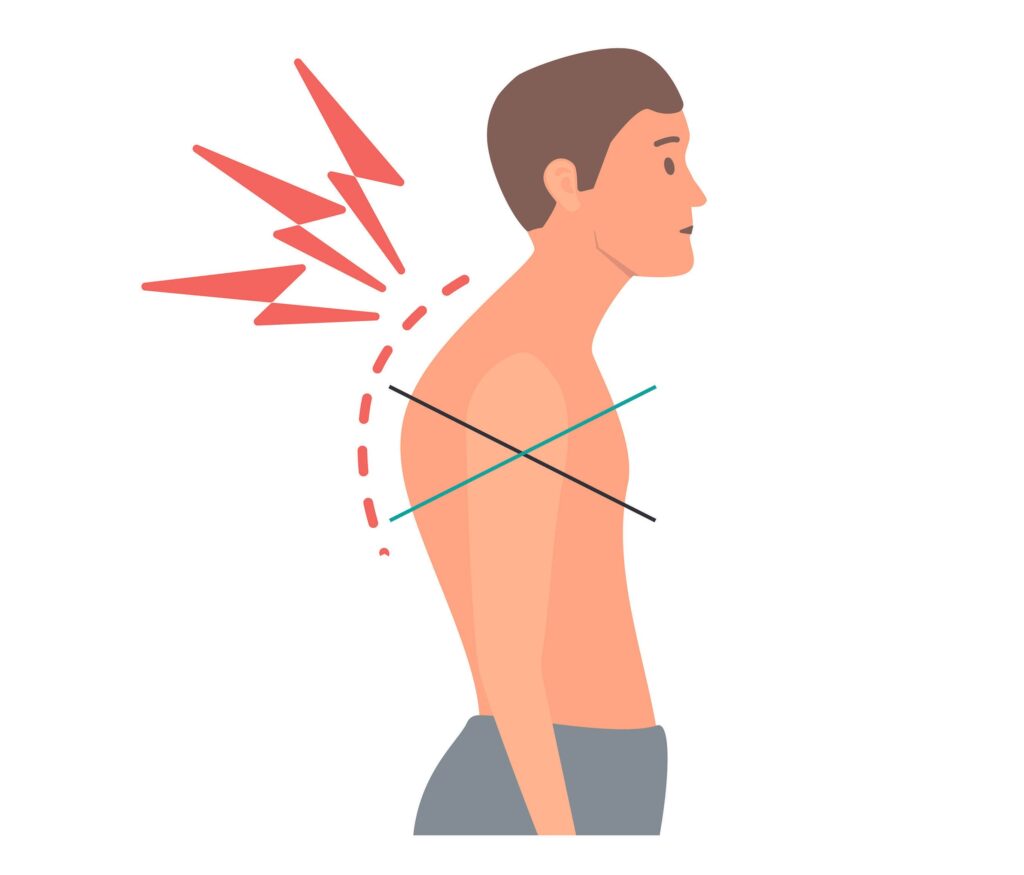
Affected Posture:
- Forward head posture
- Increased cervical lordosis (neck extension)
- Increased thoracic kyphosis (rounded upper back)
- Scapular winging or protraction
- Rounded shoulders
In UCS, mainly the posterior superior muscles in the neck and the anterior neck, which are tonic, are short and the anterior deep muscles of the neck and posterior shoulder girdle, which are mainly phasic, are inhibited and weakened.
Causes and Risk Factors
- Prolonged poor posture, especially during desk work or device use
- Sedentary lifestyle
- Imbalanced training (e.g., excessive chest workouts without back strengthening)
- Repetitive forward-head movement patterns
- Occupational risks (office workers, drivers, students, etc.)
Affected Joints
- Atlanto-occipital joint
- Cervicothoracic junction
- Glenohumeral joint
- Scapulothoracic articulation
Symptoms and Clinical Signs
- Neck and shoulder pain or stiffness
- Headaches (due to muscle tension)
- Limited cervical mobility
- Numbness/tingling in the arms (if nerve impingement occurs)
- Muscle fatigue or tension in upper traps and neck
- Scapular dyskinesis (abnormal movement of the shoulder blade)
- Decreased respiratory function (due to tight pectorals)
Clinical Assessment
1. Observation & Palpation
- Postural analysis (side and back views)
- Muscle tone palpation (tightness in upper traps, levator scapulae)
2. Functional Tests
| Test | Purpose |
|---|---|
| Chin Tuck Test | Assess deep cervical flexor strength |
| Wall Angel Test | Evaluate thoracic extension, scapular control |
| Scapular Assistance Test | Identify scapular muscle dysfunction |
| Pectoralis Minor Length Test | Evaluate anterior shoulder tightness |
Janda’s Basic Movement Patterns Janda identified six basic movement patterns that provide overall information about a particular patient’s movement quality and control; these movements form the basis of the hip extension, hip abduction, curl-up, cervical flexion, push-up, and shoulder abduction movement pattern tests. The clinician should observe both the left and right sides for comparison. Muscle or limb trembling during these tests is considered a positive finding, indicating weakness or fatigue. Some patients do not need to perform all six tests at once; the clinician should decide which tests are indicated based on the postural analysis and history
Outcome Measures
- Shoulder Pain and Disability Index (SPADI)
- Neck Disability Index
- Occiput to Wall Test
- SF-36 questionnaire
- McGill-Melzack Pain Questionnaire
- Visual analogue scale (VAS)
Differential Diagnosis
| Condition | Distinguishing Feature |
|---|---|
| Thoracic Outlet Syndrome | Neurovascular symptoms with arm elevation |
| Cervicogenic Headache | Unilateral head pain from cervical spine |
| Myofascial Pain Syndrome | Trigger points present |
| Shoulder Impingement | Painful arc, weakness in rotator cuff muscles |
Management / Interventions
Physical therapy Interventions inludes:
a. Inhibit/Treat Tight Muscles (Overactive)
- Soft tissue release (manual therapy, myofascial release)
- Stretching:
- Pectoralis major & minor
- Upper trapezius
- Levator scapulae
- SCM
b. Activate & Strengthen Weak Muscles (Underactive)
- Strengthening exercises:
- Deep cervical flexors: Chin tucks, head nods
- Lower trapezius: Prone Y raises, scapular retraction
- Serratus anterior: Wall slides, push-up plus
- Rhomboids: Rows
c. Postural Re-education
- Ergonomic corrections (desk, screen, chair height)
- Mirror or video feedback
- Bracing or taping (if needed for short-term support)
d. Motor Control and Functional Integration
- Incorporate strengthening into daily tasks
- Functional reaching or lifting with correct posture
- Breathing exercises for diaphragm recruitment
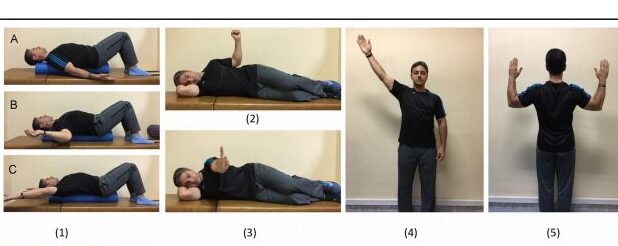
There have been some studies showing effective exercise programmes for people with UCS, and one of these is Comprehensive corrective exercise program (CCEP), Below is the list of exercises used in the CCEP:
Prevention Strategies
- Ergonomic workspace setup
- Regular posture checks during prolonged sitting
- Active breaks every 30–45 minutes
- Balanced strength training routine (avoid push-dominant programs)
- Incorporate mobility and stability drills in warm-ups
“Upper Cross Syndrome is not a diagnosis, but a descriptive pattern. A full assessment must rule out pathology before attributing symptoms solely to UCS.”


Pingback: Lower Cross Syndrome: its causes| risk factors| treatment everything you need to know - Nutriphyfit